Medical Records Request Form Template
Medical Records Request Form Template - Web write a medical records release authorization letter to the relevant office requesting the release, access, or transfer of health information. Web a medical records release authorization form is a document that allows healthcare providers to share a patient's medical records with specified parties, such as insurance companies or other doctors. Web the hipaa medical record release form allows you to identify those individuals to whom you would like your medical information disseminated and protect your information from unauthorized persons. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Web free medical records release (authorization) form templates. This form should comply with the health insurance portability and accountability act (hipaa). Our medical record request form is easily accessible in word, pdf, and google docs formats, making it a convenient choice for different needs. Web whether you’re a doctor, nurse, physical therapist, or other medical professional, easily collect your patient’s medical history using this free medical history form. Jotform’s medical records release authorization template allows you to quickly and easily gather signatures from patients or parents or guardians in order to release sensitive medical records to. Web a medical records release form is a document that permits a medical office to disclose a patient’s protected health information. Web our template captures all these crucial details, facilitating an efficient process to access medical records. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. This makes it easy to request the records needed to validate your injury claim. All you need to do is customize the form to match how you want. Grant access to your. Web the hipaa medical record release form allows you to identify those individuals to whom you would like your medical information disseminated and protect your information from unauthorized persons. Some providers make it possible for their patients to access their medical records through a portal, and others issue a free release authorization template to be completed and sent via email,. This medical records request document is used by a patient to request that a healthcare provider who has treated them release their medical records to a specific recipient. Web the hipaa medical record release form allows you to identify those individuals to whom you would like your medical information disseminated and protect your information from unauthorized persons. Who is the. I,_____________________________________________, give my permission for ______________________________________________ to share the information listed in section ii of this document with the person(s) or organization(s) i have specified in section iv of this document. Web to request release of medical information please complete and sign this form. Web this form is for use when such authorization is required and complies with the health. This medical records request document is used by a patient to request that a healthcare provider who has treated them release their medical records to a specific recipient. Web our template captures all these crucial details, facilitating an efficient process to access medical records. Patients should consider the recipient and the information required. I, ____________________________________hereby voluntarily authorize the disclosure of. If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your protected health information or request a change to your health record. Download this medical record request letter and fill in the blanks. Web a hipaa release form must be obtained from a. This medical records request document is used by a patient to request that a healthcare provider who has treated them release their medical records to a specific recipient. Web choosing the best type of hipaa form is important to authorize an individual, medical professional, billing office, or insurance representative to release or view medical records. All you need to do. Our medical record request form is easily accessible in word, pdf, and google docs formats, making it a convenient choice for different needs. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Utilize the proven template to get you started. Web write a medical records release authorization letter to the relevant office requesting the release, access, or. It also allows the added option for healthcare providers to share information. Web need a medical records release form for your medical practice? Web whether you’re a doctor, nurse, physical therapist, or other medical professional, easily collect your patient’s medical history using this free medical history form. Web a hipaa release form must be obtained from a patient before their. Web commonly, ways to get your medical records will depend on your health care provider’s process. Jotform’s medical records release authorization template allows you to quickly and easily gather signatures from patients or parents or guardians in order to release sensitive medical records to. I,_____________________________________________, give my permission for ______________________________________________ to share the information listed in section ii of this. Web download a medical records release (hipaa) form to authorize healthcare providers to release medical information. Web commonly, ways to get your medical records will depend on your health care provider’s process. Some providers make it possible for their patients to access their medical records through a portal, and others issue a free release authorization template to be completed and sent via email, mail, or fax. Grant access to your protected health information. Download this medical record request letter and fill in the blanks. Web this form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. This makes it easy to request the records needed to validate your injury claim. Web whether you’re a doctor, nurse, physical therapist, or other medical professional, easily collect your patient’s medical history using this free medical history form. It also allows the added option for healthcare providers to share information. All you need to do is customize the form to match how you want. I,_____________________________________________, give my permission for ______________________________________________ to share the information listed in section ii of this document with the person(s) or organization(s) i have specified in section iv of this document. Web our template captures all these crucial details, facilitating an efficient process to access medical records. A medical records release form is a document used to authorize the transfer of a patient's medical records from one healthcare provider to another. Our medical record request form is easily accessible in word, pdf, and google docs formats, making it a convenient choice for different needs. Web choosing the best type of hipaa form is important to authorize an individual, medical professional, billing office, or insurance representative to release or view medical records. Clearly state which records you need, including dates of service, types of records, and any other specific details.
Medical Records Request form Template Fresh Medical Records Release

Printable Medical Record Request Form Template Printable Templates
Printable Medical Record Request Form Template Printable Templates

Medical Record Request Form Template Addictionary
Printable Medical Record Request Form Template Printable Templates
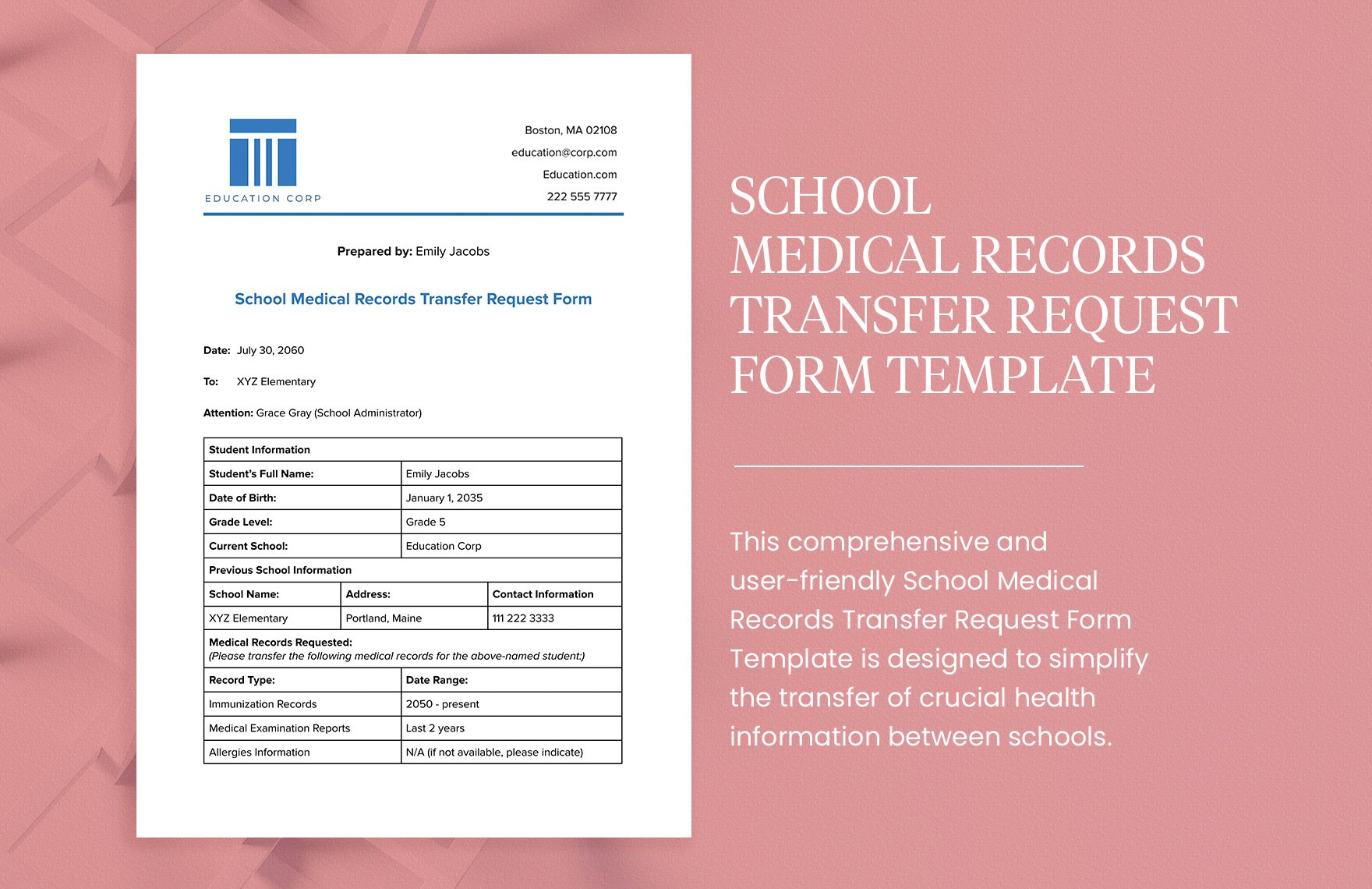
School Medical Records Transfer Request Form Template in PDF, Word
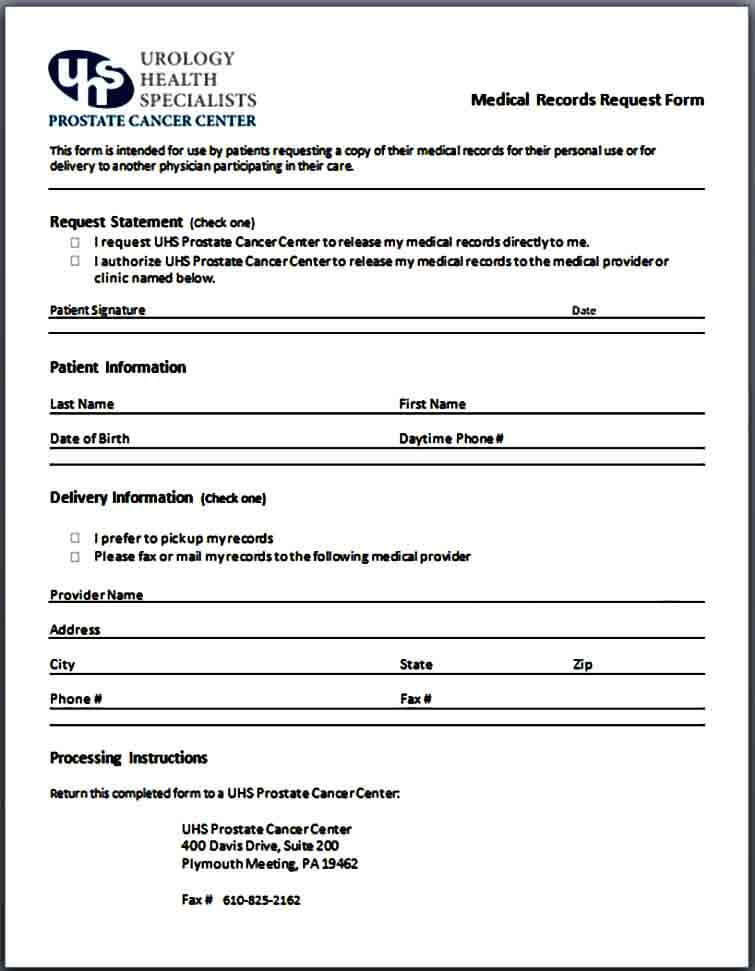
Sample Medical Records Request Form Mous Syusa
Sample Medical Records Request Form Mous Syusa
11+ Medical Records Release Forms Samples, Examples & Format Sample
Medical Records Request Form Template
Who Is The Person Making This Request For Medical Records?
Web Download A Basic Template (Free) Create A Customized Document.
Medical Records Request For ________ Dear ________, I Am A Current Patient Of ________ Asking That You Provide Me With A Copy Of My Medical Records From.
Web Write A Medical Records Release Authorization Letter To The Relevant Office Requesting The Release, Access, Or Transfer Of Health Information.
Related Post: