Medical Necessity Appeal Letter Template
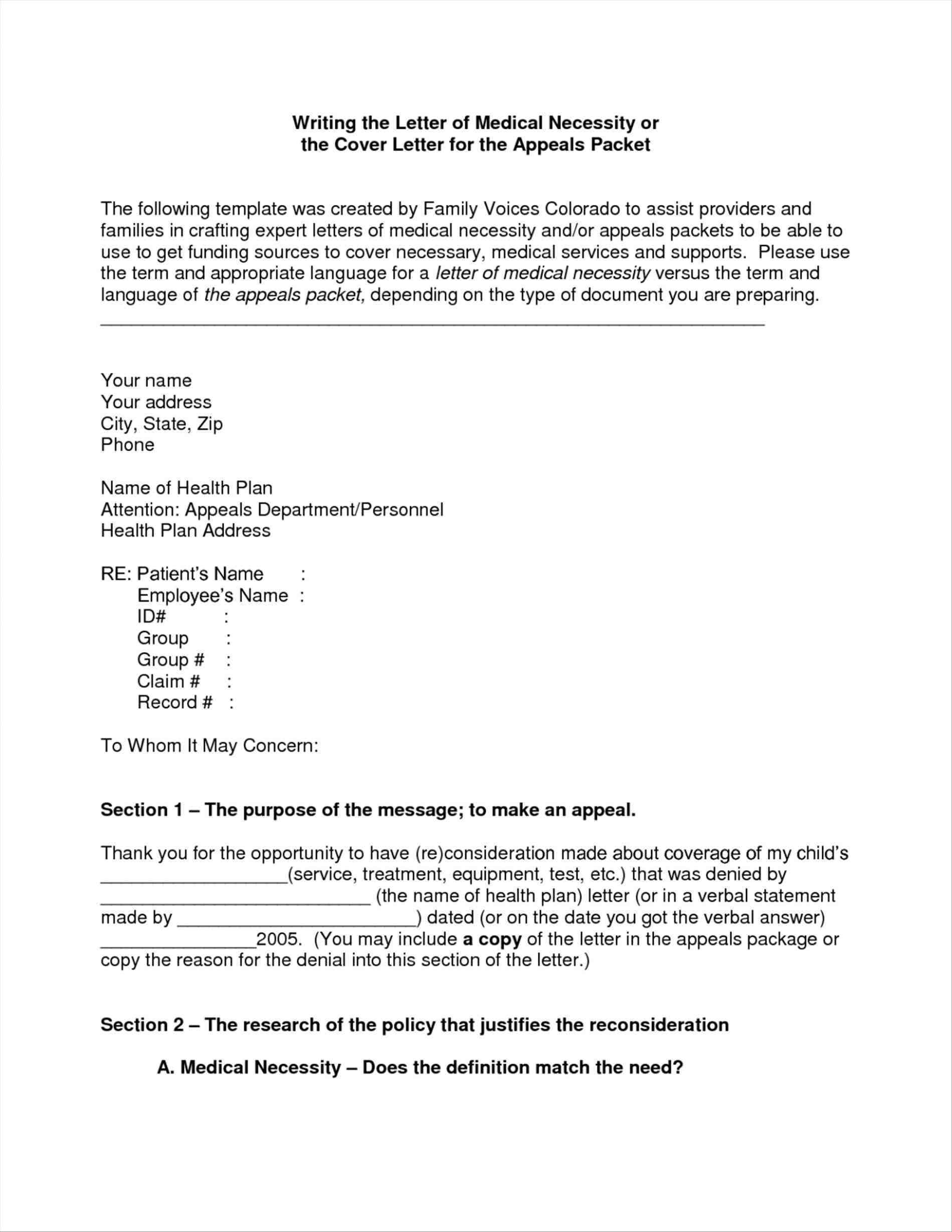
Medical Necessity Appeal Letter Template - This customizable ms word and google. Ask your medical provider to prepare a letter of medical necessity explaining prior treatments, the reason the treatment in question is being. Web so, if time is the leading factor as to why your organization doesn’t send appeal letters for your medical claim denials, what should you do? To most effectively write an appeal letter, follow these steps: I am writing this letter to appeal for the coverage of orthodontic. Your doctor has ordered a bilateral digital breast tomosynthesis, a screening mammogram,. Write an appeal letter that addresses the issues in the health plan’s denial letter. The purpose of an lmn is for a healthcare provider to provide reasoning as to why a certain medication, like contrave, is medically. Web letter of medical necessity (lmn). * as medical necessity criteria for transitional case management requires the child to. [health plan] denied payment for services. To most effectively write an appeal letter, follow these steps: Web many health plans require that a letter of medical necessity (lmn) accompany an appeal letter. Fields required for customization are in red. Web your appeal should include: Below are three unique templates to guide you in writing an. A letter from your doctor and specialist addressing specifics of your case. I am writing, on behalf of [name of plan member if other than yourself], to appeal the [name of health plan and policy number] decision to deny [name. Web sample letter of medical necessity/ appeal template cover. Web please customize the appeal letter template based on the medical appropriateness. Web many health plans require that a letter of medical necessity (lmn) accompany an appeal letter. Web many health plans require a letter of medical necessity when appealing a coverage determination or prior authorization for a patient’s plan.* the purpose of a letter of. Fields required for customization. To most effectively write an appeal letter, follow these steps: You need to make a. The purpose of an lmn is for a healthcare provider to provide reasoning as to why a certain medication, like contrave, is medically. Web many health plans require a letter of medical necessity when appealing a coverage determination or prior authorization for a patient’s plan.*. Web cite plan language where possible. Your company has denied this claim for the following. * as medical necessity criteria for transitional case management requires the child to. Web practicing doctors use a letter of medical necessity template when preparing a letter to insurance companies to prove that a patient requires medical. Web physicians can reference this publication to learn. You need to make a. It is important to provide the most complete. I am writing to request a review of a denial for [patient name] for [medication] treatment. Web practicing doctors use a letter of medical necessity template when preparing a letter to insurance companies to prove that a patient requires medical. Any pertinent information from your medical records. Web an appeal letter for medical necessity is a written request for reconsideration or review of a health insurance claim or a coverage decision made by a health insurance provider. To most effectively write an appeal letter, follow these steps: You need to make a. A letter from your doctor and specialist addressing specifics of your case. Web so, if. It is important to provide the most complete. A letter from your doctor and specialist addressing specifics of your case. Fields required for customization are in red. This customizable ms word and google. Web many health plans require that a letter of medical necessity (lmn) accompany an appeal letter. To most effectively write an appeal letter, follow these steps: This customizable ms word and google. Web above medical necessity criteria have not been met may result in recoupment. Write an appeal letter that addresses the issues in the health plan’s denial letter. The following pages are a template that may be customized to use as a statement of medical. [health plan] denied payment for services. Web letter of medical necessity (lmn). A letter from your doctor and specialist addressing specifics of your case. Web the appeal letter should be clear, concise, and structured, emphasizing the medical necessity of the treatment. Web dear medical or pharmacy director: Web so, if time is the leading factor as to why your organization doesn’t send appeal letters for your medical claim denials, what should you do? Web cite plan language where possible. You need to make a. Web sample letter for a “not medically necessary” and “investigational” denial. Your doctor has ordered a bilateral digital breast tomosynthesis, a screening mammogram,. * as medical necessity criteria for transitional case management requires the child to. Web practicing doctors use a letter of medical necessity template when preparing a letter to insurance companies to prove that a patient requires medical. Web dear [insurance provider name], i hope this letter finds you in good health and high spirits. Web letter of medical necessity (lmn). [health plan] denied payment for services. It is important to provide the most complete. Any pertinent information from your medical records. The purpose of an lmn is for a healthcare provider to provide reasoning as to why a certain medication, like contrave, is medically. Web many health plans require a letter of medical necessity when appealing a coverage determination or prior authorization for a patient’s plan.* the purpose of a letter of. I am writing to request a review of a denial for [patient name] for [medication] treatment. Web introducing our free medical necessity appeal letter template, designed to assist you in advocating for essential medical treatments.
Medical Necessity Appeal Letter Template
Letter of Medical Necessity Template Download Printable PDF
![Free Printable Letter Of Medical Necessity Templates [PDF, Word]](https://www.typecalendar.com/wp-content/uploads/2023/07/Blank-Letter-of-Medical-Necessity-Word.jpg?gid=695)
Free Printable Letter Of Medical Necessity Templates [PDF, Word]
Appeal Letter Template For Medical Necessity Get What You Need For Free

Medical Appeal Letter Sample Templates Sample Templates
Medical Necessity Appeal Letter Template Download Printable PDF
Appeal Letter Template For Medical Necessity Get What You Need For Free

Medical Necessity Appeal Letter Template Pdf
Appeal Letter Template For Medical Necessity Get What You Need For Free

Medical Necessity Appeal Letter Template
A Letter From Your Doctor And Specialist Addressing Specifics Of Your Case.
I Am Writing, On Behalf Of [Name Of Plan Member If Other Than Yourself], To Appeal The [Name Of Health Plan And Policy Number] Decision To Deny [Name.
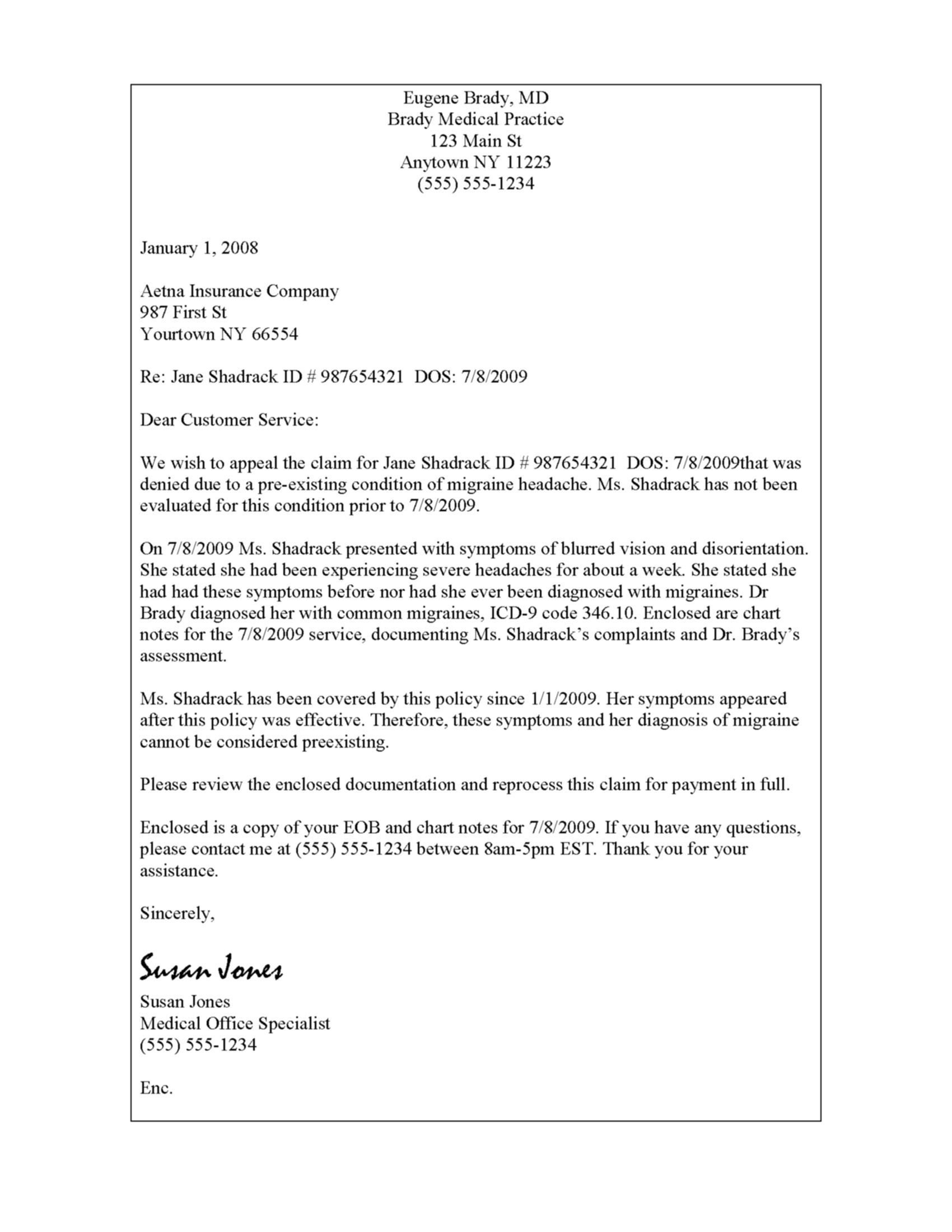
Web An Appeal Letter For Medical Necessity Is A Written Request For Reconsideration Or Review Of A Health Insurance Claim Or A Coverage Decision Made By A Health Insurance Provider.
Web Many Health Plans Require That A Letter Of Medical Necessity (Lmn) Accompany An Appeal Letter.
Related Post: